Dr Elizabeth Radford, CUH
Definition

Drug-resistant epilepsy with multiple seizure types
- Onset prior to 18 years
- Most common / must have tonic seizures
- Other types: atypical absences, drop attacks
- Less common: clonic, myoclonic, GTCS

Accompanying cognitive impairment & potentially behavioural impairment (not necessarily present at seizure onset)

EEG: diffuse slow spike-and-slow-wave <2.5 Hz and generalised paroxysmal fast activity >10 Hz in sleep
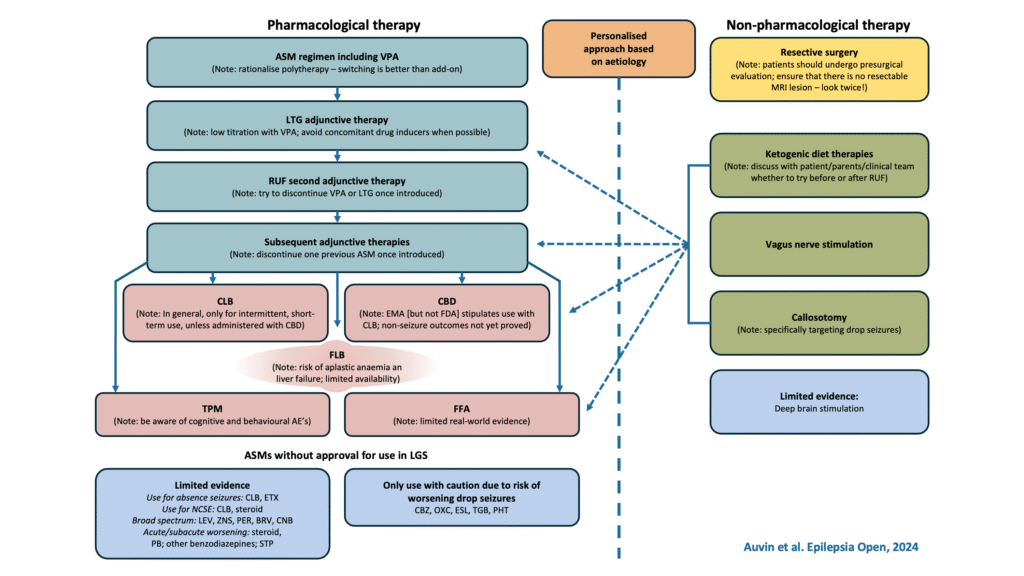
How to manage LGS
- Be careful in setting appropriate goals (seizure burden vs risk of side-effects)
- ‘Personalised’ approach
- Discuss with tertiary colleagues/MDT
- Combination of medications (beware polypharmacy), dietary options, surgical options

Guidance
1st line
Sodium Valproate
2nd line
Lamotrigine
3rd line
Rufinamide / Clobazam / CBD
4th line
Ketogenic diet
March 2025 – fenfluramine approved as add-on (3rd line)
Cenobamate might also be considered afterwards